
Thursday, September 6, 2012
Myotonia Dystrophica

Charecteristics are-expressionles face due to wasting of facial and temporal muscles,called myopathic face.
Swan-like neck due to wasting of sternocleidomastoids.
Tuesday, August 14, 2012
Thalassemias

Hemoglobin Synthesis
Hemaglobin is a tetramer protein (meaning it has 4 heme groups)
2 alpha protein subunits & 2 Beta protein subunits
There is an iron atom in the center of each heme group
Function: Reversible binding of Oxygen
Thalessemias are the MOST common genetic disease worldwide. They are a group of disorders with ineffective RBC production (impairment in rate of globin chain synthesis) resulting in microcytic anemai with ineffective erythropoiesis.
Inherited defect in Beta chain synthesis
Unaffected alpha chain continues to be produced and accumulates in the RBC and interferes with normal maturation and contributes to the RBC destruction. The excess alpha chains denature to form precipitates called Heinz bodies in the RBC precursors in the boen marrow. The Hdinz bodies impair DNA synthesis & damage the RBC membrane which can lead to severe hypochromic microcytic anemia.
Chronic transfusions are required with an inevitable iron overload. 50% of untreated patients die by 5 years of age.
Clinical Manifestations
The more severe the imbalance between alpha & beta hemoglobin the worse the disease
Heterozygous = Beta Thalassemia Minor (mose normal Hgb and malarial protection)
Homozygous = Beta Thalassemia Major (severe, transfusion-dependent, early onset at 6-9 months of age, growth retardation)
Every body system is affected
- increased hematopoiesis leads to bone marrow expansion, impaired growth & thinning of cortical bone
- increased red cell destruction leads to increased iron absorption, splenomegaly & hepatomegaly (fibrosis, cirrhosis)
- Heart: arrhythmia, myocarditis, congestive heart failure
- Pancrease: Beta cells are destroyed leading to diabetes
- Pituitary: growth retardation, hypogonadotropic hypogonadism
- Parathyroid: hypocalcemia, osteoporosis
- Frontal bossing/severe thalassemia facies (see photo below)
- hepatosplenomegaly
- hypersplenism
- pallor
- cachexia
- fatigue
- poor appetite

The x-ray on the right above demonstrates bone marrow hyperplasia of the skull.
Laboratory Features
Severe anemia with MCV in the 50-60 range (microcytosis) also hypochromic
On smear will be target cells and hardly any normal cells
Treatment
Regular Transfusions
Folate supplementation
Spenectomy (for hypersplenism) as indicated by:
Severe anemia with MCV in the 50-60 range (microcytosis) also hypochromic
On smear will be target cells and hardly any normal cells
Treatment
Regular Transfusions
- Hgb goal post ransfusion of 10g/dl
- needed approximately every 4 weeks
- Desferoxamine (Desferal)
- SQ over 10-12 hours, 5-6 days/wk
- avoid if < 3 years old because of toxicity
- Side effects: ototoxicity with high frequency hearing loss, retinal changes, bone dysplasia/truncal shortening
Folate supplementation
Spenectomy (for hypersplenism) as indicated by:
- Dramatic increase in transfusion requirements
- massive size that interfres with breathing and nutrition
- severe pain
- avoid before 5 years if at all possible
- immunize with pneumovax and menigovax pre-splenectomy
- post splenectomy will need penicillin prophylaxis for life
Friday, August 10, 2012
Marasmus

Checklist of points for conducting the physical examination
- Body temperature (measured with a thermometer) - Allowing measurement of low temperatures to detect hypothermia as well as fever
- Anemia - Pale mucosa
- Edema
- Dehydration - Thirst, shrunken eyes
- Hypovolemic shock - Weak radial pulse, cold extremities, decreased consciousness
- Tachypnea - Pneumonia, heart failure
- Abdominal manifestations - Distension, decreased or metallic bowel sounds, large or small liver, blood or mucus in the stools
- Ocular manifestations - Corneal lesions associated with vitamin A deficiency
- Dermal manifestations - Evidence of infection, purpura
- Ear, nose, and throat (ENT) findings - Otitis, rhinitis

Allergic Rhinitis

Allergen mediated; thus, allergen avoidance is the best treatment.
➤ Nasal steroids are the most effective chronic allergic rhinitis medications, often used with antihistamines.
➤ Nasal polyps can be sequelae of chronic inflammation and allergic rhinitis, but younger patients with polyps must be screened for cystic fibrosis.
People often confuse an allergy with a cold or flu. Remember colds are short-lived and passed from person to person, whereas allergies are immune system reactions to normally harmless substances
Low Backache

In 90% of patients,acute low back pain,even with sciatic nerve involvement, resolves within 4 to 6 weeks.
➤ Analgesics, such as nonsteroidal anti-inflammatory drugs or narcotics, muscle relaxants, and attempts at maintaining some level of activity are helpful in managing acute low back pain; bedrest does not help.
➤ Pain that interferes with sleep, significant unintentional weight loss, or fever suggests an infectious or neoplastic cause of back pain.
➤ Imaging studies, such as magnetic resonance imaging, are useful only if surgery is being considered (persistent pain and neurologic symptoms after 4 to 6 weeks of conservative care in patients with herniated disks) or
if a neoplastic or inflammatory cause of back pain is being considered.

Pericardial Effusion and Cardiac Tamponade ,the difference :
PERICARDIAL EFFUSION: Fluid that fills the pericardial space, which may be due to infection or malignancy. A rapid accumulating effusion may lead to cardiac compromise.
CARDIAC TAMPONADE: Increased pressure within the pericardial space caused by an accumulating effusion, which compresses the heart and impedes diastolic filling.
Cystic Fibrosis

CYSTIC FIBROSIS (CF): The major cause of chronic debilitating pulmonary disease and pancreatic exocrine deficiency in the first three decades of life. It is characterized by the triad of chronic obstructive pulmonary disease, pancreatic exocrine deficiency, and abnormally high sweat electrolyte concentrations.
Characteristic pancreatic changes give the disease its name.
➤ Cystic fibrosis (CF) involves a defect in mucus secretion and eccrine sweat gland function, resulting in various visceral lumina obstructions and excessive electrolyte secretion.
➤ Extrapulmonary signs and symptoms, such as digital clubbing, recurrent sinusitis, growth retardation, and fat malabsorption, are clues to the diagnosis of cystic fibrosis.
➤ A negative sweat chloride test result does not preclude cystic fibrosis.
➤ Meconium ileus in the newborn period is nearly pathognomonic for cystic fibrosis
Vestibulo-Ocular Reflex

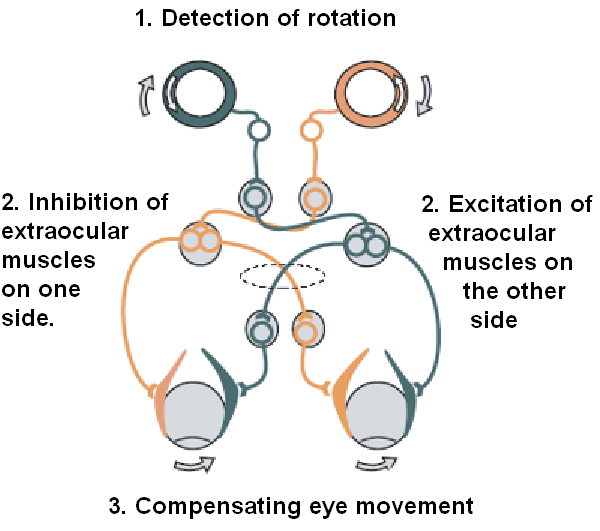

doll's eye reflex
symmetrical deviation of the eyes when the head is moved in different positions, always returning to center. Abnormalities are caused by lesions of the inner ear or brainstem, especially the pons and midbrain. Called also oculocephalogyric reflex, oculovestibulocephalic reflex. Called also doll's head reflex.
The VOR is ultimately driven by signals from the vestibular apparatus in the inner ear. The semicircular canals detect head rotation and drive the rotational VOR, whereas the otoliths detect head translation and drive the translational VOR. The main "direct path" neural circuit for the horizontal rotational VOR is fairly simple. It starts in the vestibular system, where semicircular canals get activated by head rotation and send their impulses via the vestibular nerve (cranial nerve VIII) through Scarpa's ganglion and end in the vestibular nuclei in the brainstem. From these nuclei, fibers cross to the contralateral cranial nerve VI nucleus (abducens nucleus). There they synapse with 2 additional pathways. One pathway projects directly to the lateral rectus of eye via the abducens nerve. Another nerve tract projects from the abducens nucleus by the medial longitudinal fasciculus to the oculomotor nuclei, which contain motorneurons that drive eye muscle activity, specifically activating the medial rectusmuscles of the eye through the oculomotor nerve.
Another pathway (not in picture) directly projects from the vestibular nucleus through the ascending tract of Dieters to the ipsilateral medial rectus motoneuron. In addition there are inhibitory vestibular pathways to the ipsilateral abducens nucleus. However no direct vestibular neuron to medial rectus motoneuron pathway exists.
Similar pathways exist for the vertical and torsional components of the VOR.
In addition to these direct pathways, which drive the velocity of eye rotation, there is an indirect pathway that builds up the position signal needed to prevent the eye from rolling back to center when the head stops moving. This pathway is particularly important when the head is moving slowly, because here position signals dominate over velocity signals. David A. Robinson discovered that the eye muscles require this dual velocity-position drive, and also proposed that it must arise in the brain by mathematically integrating the velocity signal and then sending the resulting position signal to the motoneurons. Robinson was correct: the 'neural integrator' for horizontal eye position was found in the nucleus prepositus hypoglossi in the medulla, and the neural integrator for vertical and torsional eye positions was found in the interstitial nucleus of Cajal in the midbrain. The same neural integrators also generate eye position for other conjugate eye movements such as saccades and smooth pursuit.
This reflex can be tested by the Rapid head impulse test or Halmagyi-Curthoys-test, in which the head is rapidly moved to the side with force, and is controlled if the eyes succeed to remain looking in the same direction. When the function of the right balance system is reduced, by a disease or by an accident, quick head movement to the right cannot be sensed properly anymore. As a consequence, no compensatory eye movement is generated, and the patient cannot fixate a point in space during this rapid head movement.
Comatose patients
In comatose patients, once it has been determined that the cervical spine is intact, a test of the vestibulo-ocular reflex can be performed by turning the head to one side. If the brainstem is intact, the eyes will move conjugately away from the direction of turning (as if still looking at the examiner rather than fixed straight ahead). This is how a doll's eyes would move. So having "doll's eyes" is a sign that a comatose patient's brainstem is still intact.
Thursday, August 9, 2012

Lingual Zoster
A 72-year-old woman presented to the emergency department with white patches on the right side of her tongue and slight palsy on the right side of her face, reporting that the symptoms had developed 4 days earlier. She also reported dizziness, otalgia, nausea, and vomiting. She had no history of diabetes mellitus or immunosuppressive illnesses. Examination of the tongue revealed multiple vesicles and pustules on the right side of the tongue and soft palate

Ramsay Hunt Syn ---> Herpes Zoster ---> Geniculate body ---> facial and vestibulocochlear ---> neuritis and sensoryneural hearing loss. She should have history of chicken pox.
Ramsay Hunt Syn ---> Herpes Zoster ---> Geniculate body ---> facial and vestibulocochlear ---> neuritis and sensoryneural hearing loss. She should have history of chicken pox.
Borrowed from Jewels of Clinical Medicine: Facebook

A 30-year-old woman with known congenital heart disease presented to our clinic with a 1-year history of fatigue, hemoptysis, and progressive exertional dyspnea. On examination, the toes had mild cyanosis and marked clubbing, but the finger
s had subtle clubbing only. She was noted to have a left parasternal heave, a palpable second heart sound, and a systolic ejection murmur audible in the pulmonic area. Contrast echocardiography showed right atrial and right ventricular dilatation, an elevated mean pulmonary-artery pressure of 68 mm Hg, and bidirectional flow through a patent ductus arteriosus. In Eisenmenger's syndrome, a long-standing systemic-to-pulmonary circulatory shunt results in pulmonary hypertension and eventual bidirectional or pulmonary-to-systemic shunting of blood. When Eisenmenger's syndrome occurs in concert with a patent ductus arteriosus, deoxygenated blood from the right ventricle is delivered to the aorta distal to the left subclavian artery. The upper extremities are thus spared the effects of the shunt, whereas the lower extremities are not, resulting in differential clubbing and cyanosis
Ectopia Lentis: Marfan's Syndrome and Homocystinuria

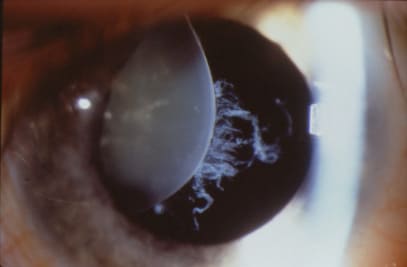

in marfan the ectopia will be up & temporal with intact zonules & partially preserved accomodation... in homocystinuriathe ectopia is inferonasal with no remaining zonular attachment
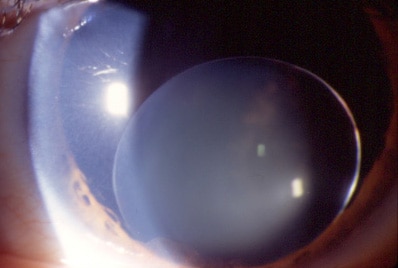
Ectopia lentis. Microspherophakia and spontaneous inferior dislocation of a lens in a patient with Weil-Marchesani syndrome.
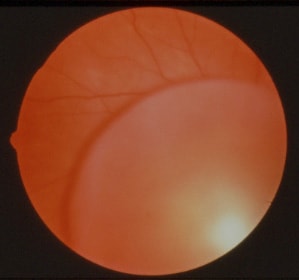
Ectopia lentis. Dislocated lens into the vitreous secondary to trauma.

Ectopia lentis. Dislocated traumatic lens (cataract).

Cavernous sinus contents
O TOM CAT:
'O TOM' are lateral wall components, in order from superior to inferior.
'CA' are the components within the sinus, from medial to lateral. CA ends at the level of T from O TOM.
· See diagram.
Occulomotor nerve (III)
Trochlear nerve (IV)
Ophthalmic nerve (V1)
Maxillary nerve (V2)
Carotid artery
Abducent nerve (VI)
T: When written, connects to the T of OTOM.

Slapped cheek disease or Fifth disease


Slapped cheek disease is a viral disease. It gets this name because, early in the infection, the child's cheeks may be bright red, as if they have been slapped. Other names for this illness are Fifth disease (there used to be six childhood rashes recognised at the turn of the century and this was the number five) and erythema infectiosum (Latin for infectious rash).
What causes it?
The causative virus is called parvovirus B 19. An Australian, Professor Yvonne Cossart first described this virus which is different from the parvovirus of dogs and cats. The virus is transmitted in droplets coughed out by infected children.
Who gets it?
Fifth disease mainly affects school and pre-school aged children, and not uncommonly causes outbreaks in schools. Most adults are immune, having already had the infection when they were children.
What does it cause?
In Fifth disease, children may get a runny nose, fever, aches and pains, and rash. At first the rash may be on the cheeks (slapped cheek appearance). After a few days a rash may be found on the arms, legs or trunk. It is pink, has a lacy appearance and may be itchy. It may fade easily, but re-appear after a bath or exercise. Older children and adults may sometimes get swollen joints (arthritis) which get better after a few days.
Can the illness be serious?
Most people get Fifth disease when they are children and cannot get it again. In most children, Fifth disease is a mild, flu-like illness, which gets better on its own in a few days.
If a pregnant woman becomes infected, the unborn baby can be severely affected. Pregnant women in contact with a child with Fifth disease should see their doctor for blood tests and monitoring of their pregnancy.
Children with haemolytic blood disorders (sickle cell anaemia, thalassaemia) and children with leukaemia can get serious problems from the virus that causes Fifth disease.
What is the treatment?
Paracetamol is useful to relieve your child's aches and pains. Your child should see a doctor if they have any swollen joints or pain not relieved by paracetamol.
Infectious period
The incubation period for this illness is approximately 1 - 2 weeks. Fifth disease is no longer infectious once the rash appears.



A CASE OF MEASLES

The characteristic measles rash is classically described as a generalized, maculopapular, erythematous rash that begins several days after the fever starts. It starts on the head before spreading to cover most of the body, often causing itc
hing. The rash is said to "stain", changing color from red to dark brown, before disappearing.The measles rash appears two to four days after initial symptoms, and lasts for up to eight days
The rubella rash is a distinctive red-pink colour. It appears 3-4 days after the first symptoms. The rash usually appears as spots, which may be slightly itchy. It usually starts behind the ears, before spreading around the head and neck. It may then spread to the trunk (abdomen and chest), legs and arms. The rash usually lasts for 3-7 days






Spider Naevi
Spider angiomas are due to failure of the sphincteric muscle surrounding a cutaneous arteriole.
The central red dot is the dilated arteriole and the red "spider legs" are small veins carrying away the freely-flowing blood. If momentary pre
ssure is applied,
it is possible to see the emptied veins refilling from the centre. No other angiomas show this phenomenon.
The dilation, in turn, is caused by increased estrogen levels in the blood.
• Many pregnant women,
• or women using hormonal contraception, have spider angiomas, due to high estrogen levels in their blood.
• People who have significant hepatic disease also show many spider angiomas, as their liver cannot detoxify estrogen from the blood, resulting in high levels of estrogen
About 33% of patients with cirrhosis have spider angiomas. As such, microhemorrhages may be observed as spider angiomas.
it is possible to see the emptied veins refilling from the centre. No other angiomas show this phenomenon.
The dilation, in turn, is caused by increased estrogen levels in the blood.
• Many pregnant women,
• or women using hormonal contraception, have spider angiomas, due to high estrogen levels in their blood.
• People who have significant hepatic disease also show many spider angiomas, as their liver cannot detoxify estrogen from the blood, resulting in high levels of estrogen
About 33% of patients with cirrhosis have spider angiomas. As such, microhemorrhages may be observed as spider angiomas.






ACROMEGALY - may be associated with HYPERTENSION, HYPERTROPHIC CARDIOMYOPATHY , VALVULOPATHY DUE TO PAPILLARY MUSCLE DYSFUCTION ,COLONIC POLYPOSIS.etc.
suppose this patient devolops infective endocarditis ->> LOOK FOR COLON POLYPS WHICH USUALLY ASSOCIATED WITH STREPTOCOCCUS BOVIS PROLIFERATION IN COLON > BACTEREMIA THUS CAUSING INFECTIVE ENDOCARDITIS OF AQUIRED MITRAL VALVULOPATHY IN ACROMEGALY....







Subscribe to:
Posts (Atom)