

doll's eye reflex
symmetrical deviation of the eyes when the head is moved in different positions, always returning to center. Abnormalities are caused by lesions of the inner ear or brainstem, especially the pons and midbrain. Called also oculocephalogyric reflex, oculovestibulocephalic reflex. Called also doll's head reflex.
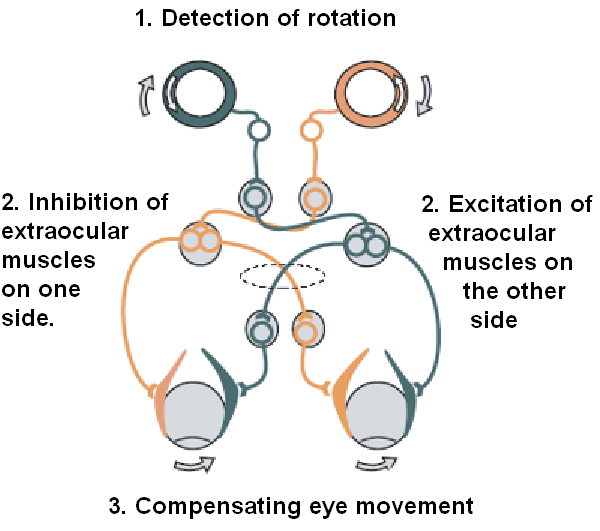
The VOR is ultimately driven by signals from the vestibular apparatus in the inner ear. The semicircular canals detect head rotation and drive the rotational VOR, whereas the otoliths detect head translation and drive the translational VOR. The main "direct path" neural circuit for the horizontal rotational VOR is fairly simple. It starts in the vestibular system, where semicircular canals get activated by head rotation and send their impulses via the vestibular nerve (cranial nerve VIII) through Scarpa's ganglion and end in the vestibular nuclei in the brainstem. From these nuclei, fibers cross to the contralateral cranial nerve VI nucleus (abducens nucleus). There they synapse with 2 additional pathways. One pathway projects directly to the lateral rectus of eye via the abducens nerve. Another nerve tract projects from the abducens nucleus by the medial longitudinal fasciculus to the oculomotor nuclei, which contain motorneurons that drive eye muscle activity, specifically activating the medial rectusmuscles of the eye through the oculomotor nerve.
Another pathway (not in picture) directly projects from the vestibular nucleus through the ascending tract of Dieters to the ipsilateral medial rectus motoneuron. In addition there are inhibitory vestibular pathways to the ipsilateral abducens nucleus. However no direct vestibular neuron to medial rectus motoneuron pathway exists.
Similar pathways exist for the vertical and torsional components of the VOR.
In addition to these direct pathways, which drive the velocity of eye rotation, there is an indirect pathway that builds up the position signal needed to prevent the eye from rolling back to center when the head stops moving. This pathway is particularly important when the head is moving slowly, because here position signals dominate over velocity signals. David A. Robinson discovered that the eye muscles require this dual velocity-position drive, and also proposed that it must arise in the brain by mathematically integrating the velocity signal and then sending the resulting position signal to the motoneurons. Robinson was correct: the 'neural integrator' for horizontal eye position was found in the nucleus prepositus hypoglossi in the medulla, and the neural integrator for vertical and torsional eye positions was found in the interstitial nucleus of Cajal in the midbrain. The same neural integrators also generate eye position for other conjugate eye movements such as saccades and smooth pursuit.
This reflex can be tested by the Rapid head impulse test or Halmagyi-Curthoys-test, in which the head is rapidly moved to the side with force, and is controlled if the eyes succeed to remain looking in the same direction. When the function of the right balance system is reduced, by a disease or by an accident, quick head movement to the right cannot be sensed properly anymore. As a consequence, no compensatory eye movement is generated, and the patient cannot fixate a point in space during this rapid head movement.
Comatose patients
In comatose patients, once it has been determined that the cervical spine is intact, a test of the vestibulo-ocular reflex can be performed by turning the head to one side. If the brainstem is intact, the eyes will move conjugately away from the direction of turning (as if still looking at the examiner rather than fixed straight ahead). This is how a doll's eyes would move. So having "doll's eyes" is a sign that a comatose patient's brainstem is still intact.
No comments:
Post a Comment